A new report from Black Book Research landed with the kind of weight that should stop healthcare IT leaders in their tracks. Issued ahead of HIMSS26 Europe in Copenhagen, it surveyed 284 hospital, health system, and cybersecurity decision-makers across the continent and arrived at a conclusion about hospital cyber resilience across Europe: cyberattacks have shifted from data theft to care disruption.
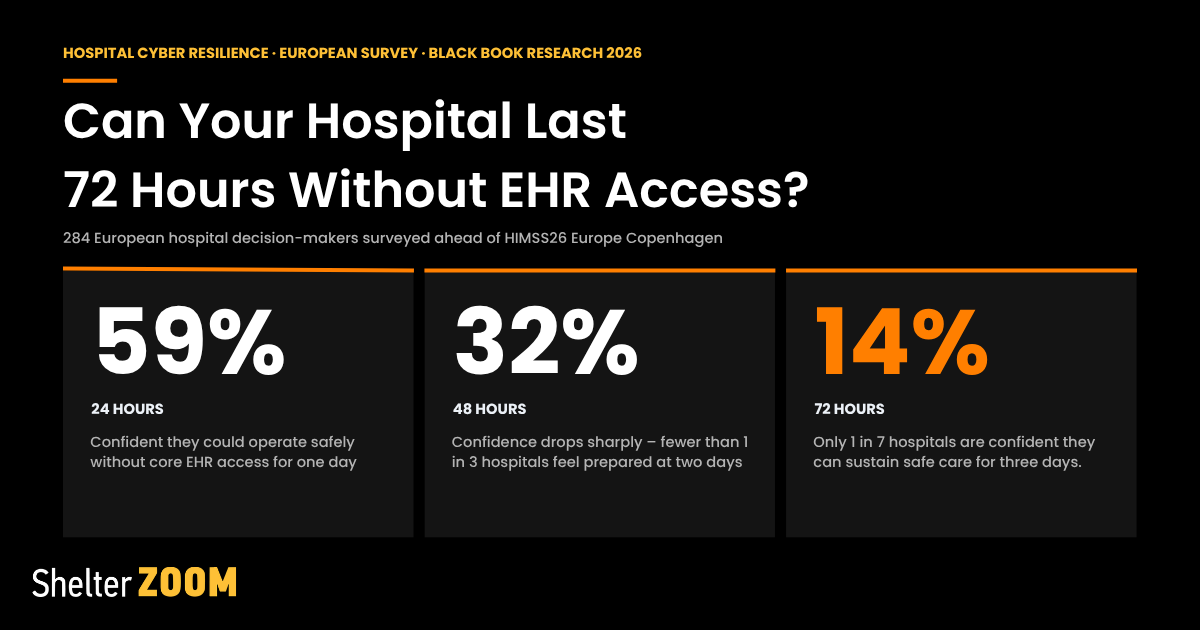
The headline statistic is stark. Only 14% of European hospital cybersecurity buyers are confident their organization can operate safely for 72 hours without core EHR access. That’s not a compliance gap. That’s a patient safety gap.
At Shelter Zoom, this report affirms what we’ve been building toward — and it sharpens the urgency for every healthcare organization evaluating their cyber readiness today.
The Threat Has Changed. Has Your Strategy?
For years, the primary fear in healthcare cybersecurity was the breach: patient records exposed, GDPR fines looming, headlines about leaked data. That threat hasn’t gone away. But attackers have gotten smarter, and the damage they can now inflict goes far deeper.
The Black Book report documents this evolution through real-world incidents most healthcare leaders will recognize. The Synnovis ransomware attack disrupted pathology services across South-East London, delaying thousands of outpatient appointments. Spain’s Hospital Clínic de Barcelona saw labs, emergency services, and pharmacy operations grind to a halt. Ireland’s HSE attack demonstrated how systemwide encryption can cascade across an entire national health infrastructure. France saw privileged-account access inside an EPR environment weaponized against sensitive patient data.
The pattern is consistent: attackers aren’t just stealing anymore — they’re shutting hospitals down.
Black Book’s Cyber Resilience Continuity Index scored the European hospital respondent group at just 44 out of 100. That number tells you everything about hospital cyber resilience in Europe today. Cybersecurity urgency is outpacing actual resilience. Organizations know the risk is real, but they aren’t yet ready to absorb the hit.
The 72-Hour Question Every Hospital Should Be Asking
The confidence cliff the report describes is a useful forcing function. Ask your team: what happens if your EHR goes dark tomorrow?
of respondents were confident they could operate for 24 hours
of respondents were confident they could operate for 48 hours
of respondents were confident they could operate for 72 hours
Only 26% had run a full clinical downtime simulation in the past 12 months. Only 25% had fully tiered critical suppliers by clinical impact and incident-response obligation.
In short, this isn’t just a technology problem. It’s a continuity planning problem — and it’s exactly where Shelter Zoom’s Spare Tire® was designed to step in.
Spare Tire is built for the moment the primary system fails. It keeps critical workflows moving during an outage, whether that’s a ransomware event, infrastructure failure, or a supplier going offline. When the EHR is down, clinical staff need somewhere to work. Spare Tire gives them that bridge — so a 72-hour outage doesn’t become a 72-hour halt in care delivery.
Documents Are the Attack Surface No One Is Watching
The press release focuses heavily on EHR and EPR systems, identity infrastructure, and network segmentation — all critical. But there’s an attack surface that gets underweighted in most cybersecurity conversations: documents.
Here’s the mechanism that gets missed: ransomware is rarely the first thing an attacker does. It’s the last. In most healthcare incidents, a compromised service account or stolen vendor credential spends days, sometimes weeks, moving quietly through clinical document repositories before encryption begins. Discharge summaries bulk-accessed at 2am. Referral batches copied to an external share by an account that has no clinical reason to touch them. These signals are detectable, but only if someone is watching document movement with the right baseline.
That’s the gap Document GPS® was built for. Most hospital security stacks monitor network traffic and endpoint behavior. Yet very few have visibility into what’s happening at the document layer — who accessed what, when, from where, and whether that pattern is consistent with how that role actually works. In post-incident investigations, the absence of that data is what turns a containable breach into a months-long forensic exercise.
The document layer isn’t just a target. In many attacks, it’s the early warning system that never got turned on.
AI-Driven Threats Require AI-Driven Defense — But Trained on the Right Baseline
The Black Book report notes that European hospital cybersecurity buyers are prioritizing MDR, XDR, and SOC modernization — with 62% citing managed detection and response as a top-demand category. Most AI-driven security tools can tell you when something looks wrong. The problem in clinical environments is that “normal” looks nothing like it does in a corporate IT network.
A nurse accessing 60 patient records in a single shift is routine. Pharmacy systems querying lab databases at 3am can be completely expected. A ward clerk printing a high volume of documents before a shift handover isn’t an anomaly — it’s a process. Generic enterprise security models flag these constantly, generating noise that drowns out the signals that actually matter. Clinical SOC teams spend enormous time chasing false positives that any experienced ward manager could have dismissed in seconds.
Mithra® AI draws from clinical workflow baselines, not enterprise IT norms. It learns the difference between a radiologist accessing PACS outside hours — which happens all the time on call — and a service account doing the same thing with no on-call assignment attached. It understands that the anomaly isn’t access volume or timing in isolation; it’s access that doesn’t fit the role, the shift pattern, or the care context.
As the Black Book report’s author put it: “Every vendor conversation should answer the same question: when the EPR is degraded, identity is compromised, the network is segmented, and a supplier is offline, can this technology help care continue safely?” That question only has a meaningful answer if the AI knows what a hospital actually looks like when it’s running normally.
CyberVault: Your Last Line of Defense
Perhaps the most critical finding in the Black Book report is also the most actionable. Of all the cybersecurity capabilities buyers are prioritizing, ransomware recovery, immutable backup, and read-only clinical access ranked third — cited by 57% of respondents. The reason it’s so high: organizations have accepted that attackers will get through. The question is how fast you can recover.
CyberVault™ is Shelter Zoom’s answer to that question. It provides secure, immutable storage for the data and credentials that matter most — isolated from the environments attackers target, preserved in a clean, recoverable state for when the attack is over. CyberVault doesn’t just store documents, it scans each one for threats before it ever makes it into the vault. Restoring from a backup only helps if what you’re restoring is clean. Reintroducing an infected document into a recovered environment can restart the entire incident.
In an environment where the average European hospital scores 44 out of 100 on clinical continuity readiness, a CyberVault deployment is the difference between a 72-hour crisis and a 72-hour recovery.
Hospital Cyber Resilience: What European Hospitals Should Do Right Now
Black Book’s recommendations for improving hospital cyber resilience are rigorous and specific. They call for 24/48/72-hour downtime simulations, live restore tests (not just checkbox reviews), validated privileged-access containment, contractually defined supplier incident obligations, and board-visible metrics tied to patient safety — not just security operations.
These are the right recommendations. But one of them deserves more scrutiny than it usually gets: the live restore test.
Most hospitals that do run restore tests are testing whether data comes back — not whether care can resume. There’s a meaningful difference. Getting a clean EHR backup onto a server is a technical milestone. However, getting nurses back into patient records, pharmacists back into medication verification, radiologists back into PACS, and ED staff back into triage workflows — with the right data, the right permissions, and the right integrations intact — is a clinical milestone. Very few organizations test for the second thing. They check the backup, not the workflow.
The implication: most business continuity plans understate their own recovery timelines, sometimes by days. The time to discover that gap is in a simulation, not at 2am during an active incident.
The nine countries Black Book identifies as cybersecurity hot zones — the UK, France, Germany, Spain, Italy, the Netherlands, Ireland, Poland, and Switzerland — represent the most digitized, most interconnected, and most operationally concentrated healthcare environments in Europe. They are targets precisely because disrupting them has maximum effect.
Black Book says 74% of European hospital buyers believe they will face a serious cyber event. Will your hospital be one of the 14% who can keep caring for patients when it happens — or one of the 86% who can’t.

Shelter Zoom Is Ready to Help
Shelter Zoom’s product suite — Document GPS, Spare Tire, Mithra AI, and CyberVault — was built around a single conviction: that healthcare organizations deserve security tools designed for the realities of clinical operations, not retrofitted from enterprise IT.
If you’re currently evaluating your hospital cyber resilience strategy, we’d welcome the conversation. The data has never been clearer about what’s at stake.